
3 results
Hyperoxia in depression
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S688-S689
-
- Article
-
- You have access
- Open access
- Export citation
Schizophrenia in Bilingual Immigrants: is Verbal Fluency Preserved in Second Language Acquisition?
-
- Journal:
- European Psychiatry / Volume 30 / Issue S1 / March 2015
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
-
Objectives
Language disturbances are the core symptoms of schizophrenia [Crow,2000]. Considering the influence of migration on the symptoms of schizophrenia [Bhugra, Gupta,2011] and few studies on the interaction of schizophrenia and bilingualism [Bersudsky, et al.,2005], we hope to clarify the linguistic profile of disorder and emphasize the role of language in schizophrenia research.
AimTo examine the linguistic features of schizophrenia in the first (L1) and the second (L2) languages, particularly in fluency as the ability to cope with native and nonnative pragmatics.
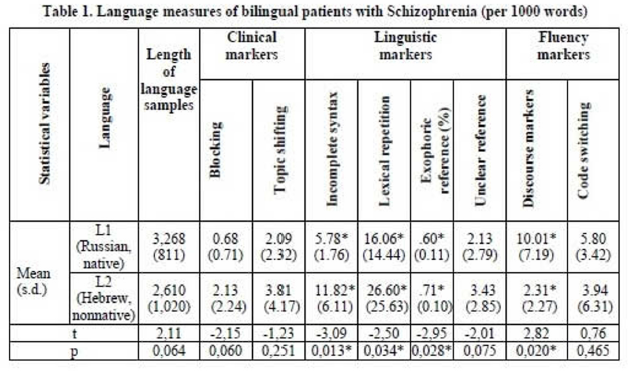
MethodsAmong sixty Russian immigrants to Israel diagnosed with schizophrenia, ten Russian-Hebrew fluent bilinguals met criteria for inclusion in the study (age: M=33.8,s.d.=11.0; length of residence: M=14.6,s.d.=6.8; time of immigration to diagnosis:M=5.3,s.d=3.9; PANSS Total score: M = 94.9,s.d = 9.8). Interviews were analyzed using clinical, linguistic and fluency speech markers. Statistical evaluation included t-test for dependent samples, two-way ANOVA(Fisher LSD post-hoc test).
ResultsThe mean length of language samples demonstrated more productivity in L1 (Table1). Clinical speech markers associated with thought disorders were similarly represented in both languages. Linguistic markers of schizophrenia occurred more often in L2. Discourse markers, as bilingual phenomenona, reflected more dysfluency in L1.
 Conclusions
Conclusions1) The higher frequency of linguistic schizophrenia markers in L2 shows more impairments in the syntax/semantic components of language, where different neural representations may underlay the two languages in a bilingual brain damaged by schizophrenia. 2) The higher frequency of fluency markers in L1 reflects attempts to maintain verbal fluency, evidenced by the use of L2 lexical items, which afford a compensatory resource for communicative discourse in schizophrenia.

Influence of birth cohort on age of onset cluster analysis in bipolar I disorder
-
- Journal:
- European Psychiatry / Volume 30 / Issue 1 / January 2015
- Published online by Cambridge University Press:
- 15 April 2020, pp. 99-105
-
- Article
- Export citation
